
Written by Brian O’Toole
The National Institute for Health and Care Excellence (NICE) Highly Specialised Technologies (HST) programme is designed to evaluate innovative treatments for rare and complex conditions. On 19th March 2025, NICE announced several refinements to the HST routing criteria, the process through which a technology is considered to meet (or not meet) HST routing. These refinements are the result of consultation between NICE and stakeholders, in an effort to provide clarity and ensure a more efficient routing process.
Summary and implication of NICE refinements
-
- The technology must meet all 4 criteria to be routed via HST
- The criteria have been amended to provide additional clarity and explicit definitions of wording and terminology
- An HST routing assessment checklist is to be used to determine whether a technology should be routed via the HST process
- NICE will review the HST routing criteria 3 years after publication to assess the need for further refinement (though a review can be initiated sooner)
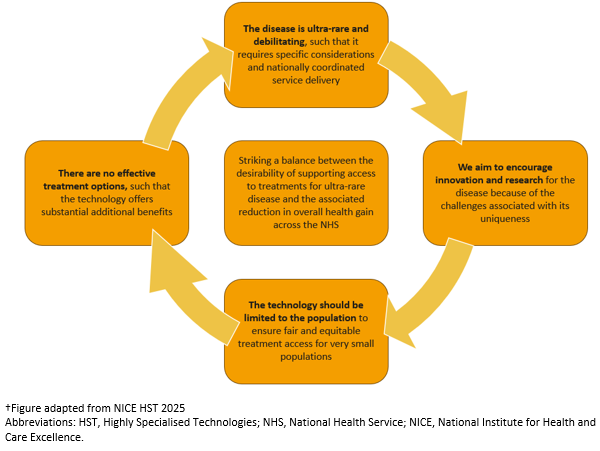
- How the context of the HST approach is linked to the HST routing criteria is presented in Figure 1, and discussed in more detail below.
Figure 1: Summary of the NICE HST Programme†
Refined NICE criteria
Routing criterion 1: The disease is ultra-rare and debilitating, that is 1A) it is defined as having a point prevalence of 1:50,000 or less in England, 1B) it is lifelong after diagnosis with current treatment and has an exceptional negative impact and burden on people with ultra-rare disease, and their carers and families
-
- ‘Disease’ refers to a condition for which a diagnosis can be made using the International Classification of Diseases (ICD-11) developed by the World Health Organization (WHO) as a guiding tool. Diagnosis is based on a unique set of signs and symptoms (characteristics) identified using using i) clinical examination; ii) patient history; iii) imaging or laboratory tests that are, or can be made, available in the National Health Service (NHS) in England.
- ‘Disease’ does not refer to subgroups based on age, sex, severity or genetic subtype. These will only be considered if they are clinically meaningful.
- ‘Point prevalence’ refers to the point prevalence of the ‘disease’ in England. It counts the number of people with a diagnosis of the disease thought to be alive in England (numerator) on a given index date compared with the total population of England (denominator) at that time (NHS England).
- ‘Lifelong’ indicates that the disease needs ongoing clinical management, supportive care, or both.
- ‘Exceptional negative impact’ refers to shortened length of life or severely impaired quality of life. The precise assessment of this will require an element of subjective judgement.
Routing criterion 2: The technology is an innovation for the ultra-rare disease
-
- ‘Innovation’ refers to a technology or medicine such as an advanced therapy medicinal product (ATMP), a new chemical or biological entity, or a novel drug device combination that brings additional health gains to people with the ultra-rare disease (compared with existing treatment or best supportive care).
- To ensure the technology is an innovation for the ultra-rare disease, the technology should not be a repurposed technology; and the indication for the technology should not be a significant extension of an indication from another population or disease.
- A repurposed technology means new uses for medicines that are outside the scope of the existing licence for the medicine. This typically involves taking an existing medicine that already has a marketing authorisation or licence for human use for a particular condition and then using it to treat another condition. This can also include generic treatments or treatments that have had marketing authorisation withdrawn and the developer is seeking a new indication.
Routing criterion 3: No more than 300 people in England are eligible for the technology and its licensed indication, and the technology is not an individualised medicine
-
- ‘Eligible’ refers to everyone who could have the technology under its marketing authorisation (obtained or in the process of being obtained) in England.
- The ‘technology’ should only be developed for the ultra-rare disease, so the eligible population is small. The technology:
-
- has to be the first licensed treatment indicated for the ultra-rare disease under consideration.
- should not be an extension of an indication (from another related population or disease, or from another subgroup of people with the same ultra-rare disease under consideration.
- is unlikely to be suitable for other subgroups of the population with the ultra-rare disease in the future who are outside of its first indication.
-
- ‘Individualised medicine’ refers to a medicine that is developed based on a person’s unique genetic profile (n of 1), or on the genetic profile of monozygotic twins or triplets.
Routing criterion 4: The technology is likely to offer substantial additional benefit for people with the ultra-rare disease over existing established clinical management, and the existing established clinical management is considered inadequate
-
- ‘Substantial additional benefit’ means that the technology is likely to significantly redress the reduced length of life or is likely to demonstrate substantial improvements in the severely impaired quality of life attributable to the ultra-rare disease, as exemplified by research data on clinically relevant measures, for example, patient-reported outcome measures (PROMs).
- ‘The technology’ means:
-
- if the technology is a disease-modifying treatment (including curative treatment), there is no other disease-modifying treatment available in the NHS in England for the same ultra-rare disease at the time of the routing decision, or
- if the technology treats a symptom or set of symptoms unique to the ultra-rare disease, there is no other treatment available in the NHS in England for the same symptom for which the technology is indicated at the time of the routing decision.
-
Conclusion
It is clear that the refinements made to the HST routing criteria add much needed clarity surrounding particular wording and terminology used by NICE. Prior to these refinements, the lack of definition meant that these criteria were subject to a considerable amount of subjectivity and interpretation. The availability of a HST routing assessment checklist provides further transparency, highlighting clearly where a technology meets, partially meets, or does not meet the criteria for routing to the HST programme. Importantly, NICE have stated that a technology must meet all 4 criteria to be considered for HST routing. Previously, it was possible for a technology that met some (but not all) to be routed.
Source Health Economics has worked with clients since 2019 to deliver ‘recommended’ NICE HST submissions, helping to ensure UK patient access to innovative treatments.
If you would like to learn more about our HTA submissions (including systematic reviews, health economic modelling, and medical writing), please contact us at Source Health Economics, a HEOR consultancy specialising in evidence generation, health economics, and communication.